The following blog is adapted from an internal email sent from our founder and CEO, Tripp Johnson, to the entire Advaita Collective, which includes Advaita Integrated Medicine and Green Hill Recovery.
We work in behavioral health, not theoretical physics. Thus most of us prefer concepts, emotions, and relationships more than data and math. I’ll skip my normal spiel on how mathematics is the universal language and jump straight into the simple math used to run an outpatient practice.
Why would I share this information? Isn’t this, like, top secret? One of our core values is transparency, and I believe that if we’re going to have a longitudinal impact on the behavioral health field, we’ve got to have an open model – one that is shared and improved upon by folks inside and outside of the Advaita Collective. I want to know if there is a better way to run this organization. By pulling back the curtain on the business model, I can improve it based on others’ input. Ultimately, we are both a business, a social enterprise, and an organization whose mission is to increase human flourishing. There is an inevitable balancing act between the utility function of patients, providers, payors, policymakers, and the company itself. (If you want to read more about the stakeholders in healthcare, check out this blog post.)
The math behind fee-for-service healthcare is deceptively simple. In a future post, I’ll dive into how providers can affect their average hourly reimbursement. I’m going to keep it pretty simple here and mainly talk about annualized revenue numbers, as the entire point of this piece is to demonstrate that consistent small misses lead to a large variance between the actual and predicted revenue. What follows applies regardless of whether you’re an in-network, out-of-network, or purely private pay provider.
revenue ($) = hours of service provided * average collections per hour ($)
Above is the entire revenue function for an individual provider or provider organization. Let’s break this down a little further to show the weekly metrics…
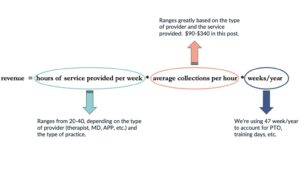
Formula clarification:
-
hours of service = hours of service scheduled – no shows
-
average collections = insurance reimbursement + copays or private payments – uncollected fees
Since most of our team has a straight salary (some folks now have a base + productivity compensation package), we will keep it simple. Note to self: it makes sense to discuss the various compensation structures we can (and do) offer and how the incentives for the organization and individual providers interact.
Revenue (In a Perfect World)

So what does this tell you? If you’re an entrepreneurial clinician, you may look at the above numbers and say, “Screw working for someone else,” however, this week, I’m only covering the revenue side of the unit economics equation. Let’s see how you feel after we check out the expense side of the equation in a few weeks.
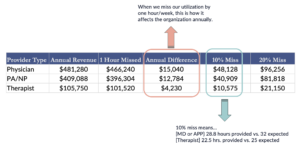
When We Come Up Short…
If an MD is expected to provide 32 hours of patient care/week and they provide 31, the company makes $15,040 less than expected annually. If it’s a 10% miss (technically 28.8 hours of service/week), the company makes $51,136 less than expected per year. And finally, if we miss utilization by 20%, the company makes a whopping $102,272 less than expected annually.
Sometimes it feels like we’re stuck between a rock and a hard place. Suppose anyone in management turns their attention to utilization. In that case, we’re perceived as uncaring. If we don’t focus on utilization, the organization continues to face the same challenges week after week because we cannot invest capital into the resources necessary to overcome the aforementioned challenges.
The discussion about utilization is not meant to minimize the toll that direct patient care takes on providers. My hope is that through presenting relevant information in a timely fashion, we can work together to accomplish our personal goals and those of the Advaita Collective.
Why does this matter? We want to have predictability in financial performance to make the appropriate investments in the organization. Last week I spent my head in the clouds talking about ikigai, and honestly, this sort of work feels close to my ikigai (communicating about marrying the money with the mission), but I digress. We cannot grow the organization, invest in individual development and training, better technology, etc., if we don’t make money. That’s just the hard truth about capitalism.
The best and worst part about my job is that my theories are constantly being challenged. Through openly discussing utilization AND how we can improve the experience for our patients and providers, we can make a lasting positive change in the health of our communities. One of my theories is simple: if we have clear expectations (agreements between providers and the organization), then everyone will feel like it’s an equitable workplace. As such, we’ve been rolling out individualized “provider agreements.”
Math is the universal language, and money is the universal medium of exchange. Compensation and revenue are just pieces of a much larger organizational calculus (business model + strategy) but are the most relevant to most of us — no one is volunteering their time, right?
A Few Additional Thoughts
Are the expectations for providers reasonable?
That’s tough for me to answer, but from talking to other folks in leadership positions in various behavioral health organizations, I believe we are providing above-average compensation for the required work. My goal is to help create upward mobility AND increased flourishing for our team members. When discussing compensation during the hiring process, I always say, “This is just a math problem.” What I mean is that compensation is highly-correlated with the expectations of the role and both sides of the equation are negotiable.
Do I think productivity or utilization is the most important metric for individuals in clinical management?
Yes and no — if the business model doesn’t work, there can be no mission.
Do I think that providers are paid enough for the services we provide?
Yes and no — some services are too highly compensated (IMHO), and many are not compensated highly enough. One of my biggest wins this year was successfully negotiating higher rates with one of the large health insurance providers.
Is increasing my productivity the only thing I can do to earn a pay raise as an individual provider in a non-management role?
No — other ways exist to increase your compensation without increasing your patient care hours. The examples above discuss general outpatient therapy and psychiatry, not specialized services such as intensive outpatient groups, full-model DBT, and more complex procedures such as TMS.
My paycheck isn’t close to what I get paid: what’s the deal?
There are significant overhead costs associated with running the Advaita Collective. I’ll do an entire post explaining the expenses associated with running an integrated care practice. Ideally, we would make everyone’s compensation public information, but we’re not there yet.