The following blog is adapted from an internal email sent from our founder and CEO, Tripp Johnson, to the entire Advaita Collective, which includes Advaita Integrated Medicine and Green Hill Recovery.
Many of us (at the Advaita Collective) worked through complex situations with our clients and their families the past couple weeks. While one case could (and should) have been avoided, I’m incredibly proud of how we handled a difficult situation.
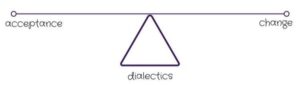
Interlude: Dialectical Theory
Thanks to being exposed to the theoretical underpinnings of dialectical behavioral therapy (DBT), I’ve become a big fan of dialectical theory. Put succinctly, dialectical theory helps us explain and navigate the apparent contradictions in daily life. I’ll be the first to admit that viewing the world through a binary, black vs. white, or wrong vs. right lens is easier. However, this type of thinking does not help us accurately understand the world. There are opposing forces at every turn. If you’re interested in learning more about dialectical theory, check out this article, Hegel’s Dialectics, or read on as I explore this week’s events and considerations through a dialectical lens.
Problem and Opportunity
We made a few errors in our admissions process. As a result, we allowed someone to enter our care that should have been screened out based on an emerging, provisional diagnosis. Ultimately, I view the situation we’re navigating as the epitome of holding the tension of conflicting truths. We made a few mistakes (problem) which allowed us to (opportunity) truly help a family navigate an emerging mental health situation. Suppose we hadn’t accepted the individual into our care. In that case, I think it’s unlikely that they would have been connected to the correct resources, ultimately resulting in better outcomes for the individual and their family.
If we’re going to make an error in judgment, I’d rather us work with individuals in a non-pathologizing manner rather than err on the side of caution. I entered this field to help people, not to mitigate risk. This article, The Problem with Planned Parenthood, explores when risk mitigation interferes with providing necessary services to folks in need.
Cultural Competency and Clinical Diagnosis
I’ll be the first to tell you I come from a privileged background. I’m an able-bodied, cis-gendered, heterosexual white guy from an upper-middle-class background and a stable familial environment. Needless to say, I’m quite lucky. That makes it even more important to educate myself extensively on cultural competency. I must go out of my way to ensure I’m fostering an inclusive environment for our team and patients. One of the “interesting” paradigms we confronted this week was the tension between pathologizing an individual, potentially without demonstrating sufficient cultural competency, while using diagnostic criteria to make the most informed decision regarding one individual’s care. While I’m a fan of adopting a transdiagnostic approach to mental healthcare, our system is (what feels like) lightyears away from it being a reality.
Too often, especially when substance misuse is involved, there can be a rush to pathologize behavior and diagnose the presenting symptoms. And for a good reason – it’s often required to receive reimbursement for treatment. There are thousands, if not millions, of folks who got a bipolar diagnosis slapped on during the early stages of treatment and recovery. Now let’s make this much more complex – add in a historically marginalized and pathologized population (young, black men) and a challenging diagnosis to wrestle with, schizophrenia.
-
Structural Racism In Historical And Modern US Health Care Policy
-
Psychiatry Confronts Its Racist Past, and Tries to Make Amends
Ultimately, we weighed the pros and cons of a patient’s clinical presentation with cultural competency. It can feel like riding a unicycle down a tightrope, but I’m very proud of how our team navigated the situation.
 Hard Truths (facts + data) and Compassionate Communication
Hard Truths (facts + data) and Compassionate Communication
 Hard Truths (facts + data) and Compassionate Communication
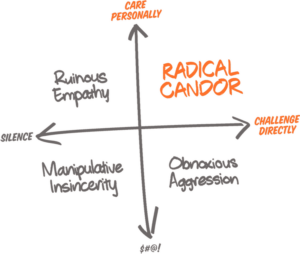
Hard Truths (facts + data) and Compassionate CommunicationWe consistently face the tension between discussing cold, hard facts and communicating with kindness. Last week, I explored how the organization must be conscious of clinical utilization if we are to complete our social mission (therein lies the tension between money and mission). With the client mentioned above, we had to honor and communicate our clinical judgment compassionately – that’s not an easy balance, especially when a family doesn’t want to accept our conclusions and recommendations. Our team (Alex, Corey, and Nick, in particular) did a phenomenal job holding a boundary with the family and extending the utmost care possible. I learned a lot about balancing a data-driven approach with kindness – the epitome of radical candor.
In Summary
I wanted to send this email last week; however, the primary situation discussed was still unfolding and felt too soon. My biggest takeaway from the past several weeks is straightforward: we have a team that goes above and beyond to serve our patients and their families. Trying to help is nice, but actually helping is the mission. We overextended ourselves in a few areas, adding more to our plates than was necessary, but I couldn’t be more proud to be part of this mission-driven team.